Field Services Portal.
A monitoring and work-order platform for Hologic's field service engineers — built to consolidate disparate tools and let engineers proactively address device issues across hundreds of healthcare sites.
Discovery
Audited the existing tool landscape — disparate systems, manual workflows, no single source of truth for FSEs in the field.
User research
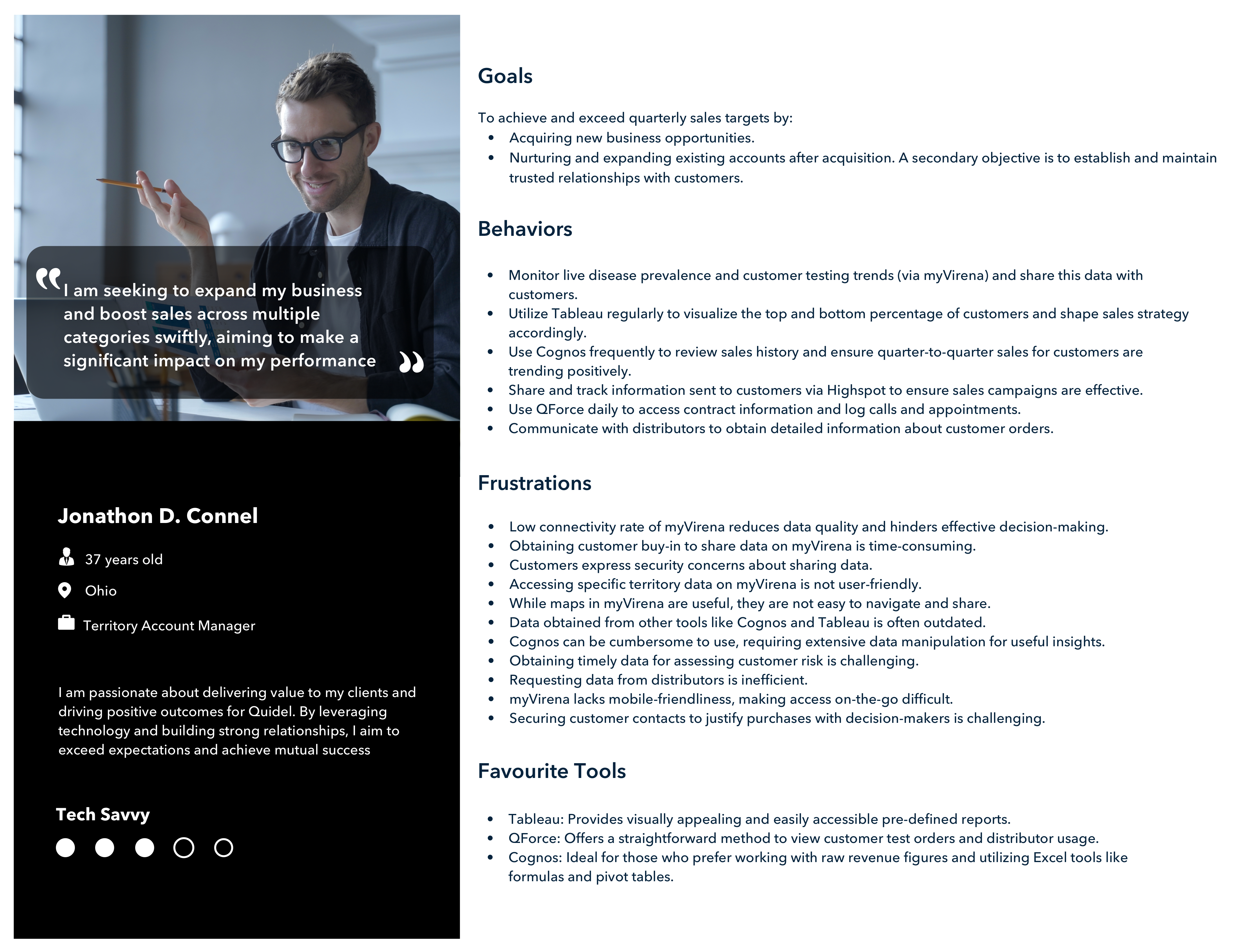
Wrote an interview script focused on values and motivations. Conducted multiple remote interviews over 5 days with the target audience.
Personas & design
Synthesized insights into personas, then designed the Portal, FSE Dashboard, and Admin Panel — collaborating with developers throughout for feasibility.
Iteration
Iterated on designs based on engineering feedback and continued user input. Research insights served as a reference point throughout.
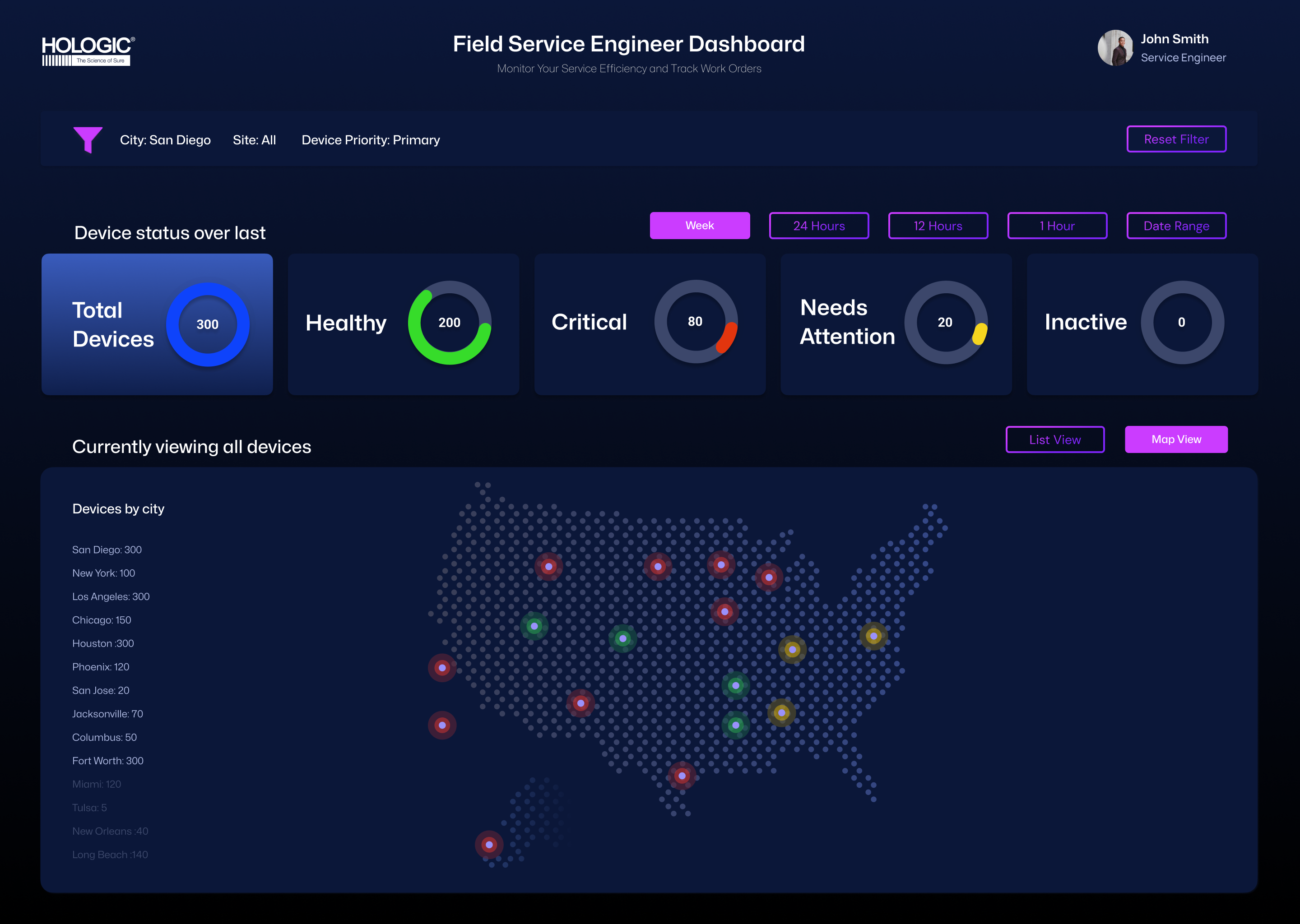
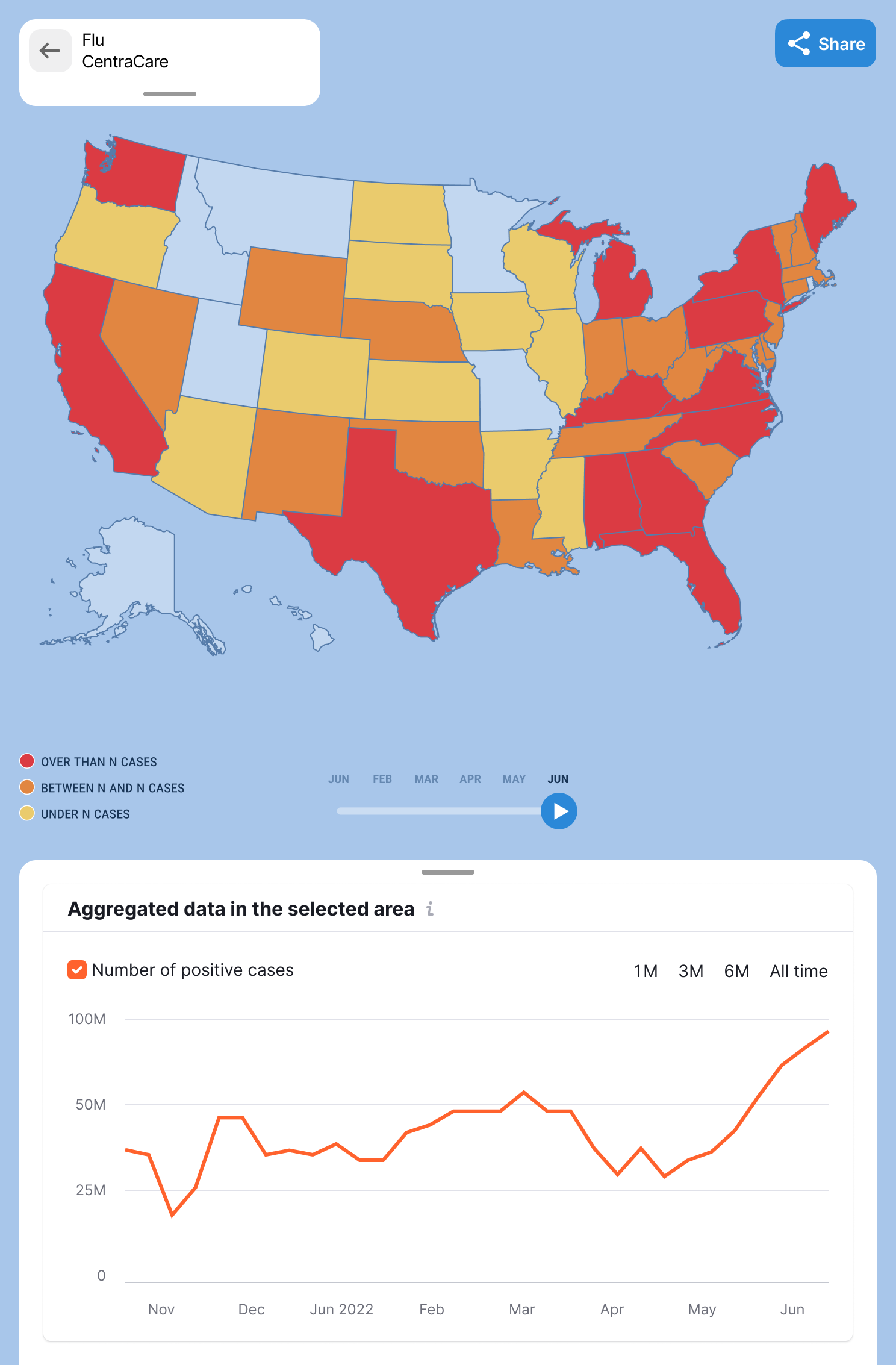
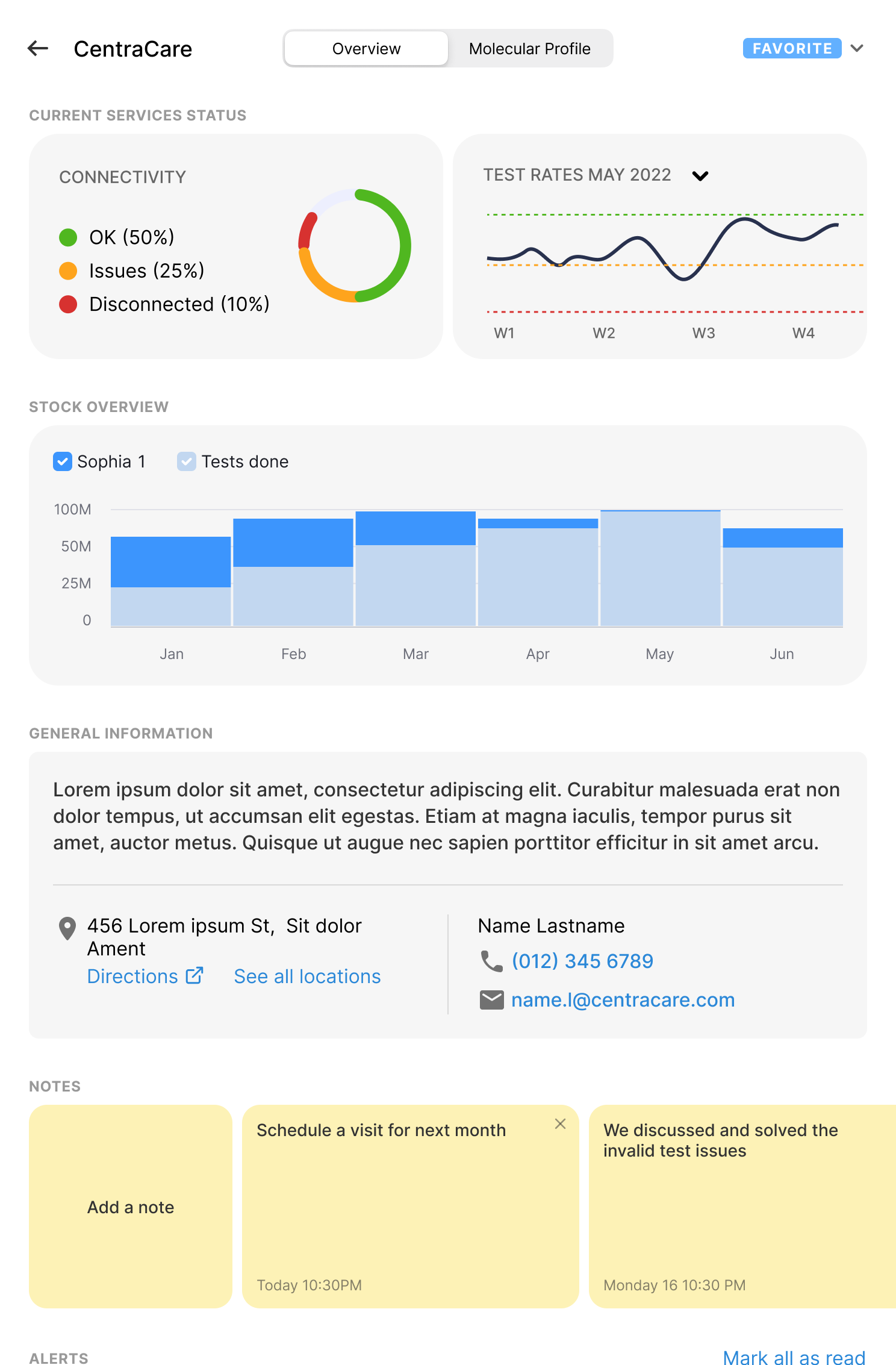
The Map View answers a question every FSE asks first: where are my devices, and which ones need attention right now? Color-coded status indicators (red for critical, yellow for warning, green for healthy) plot device locations across the US, with a city-level breakdown on the left for quick triage planning.

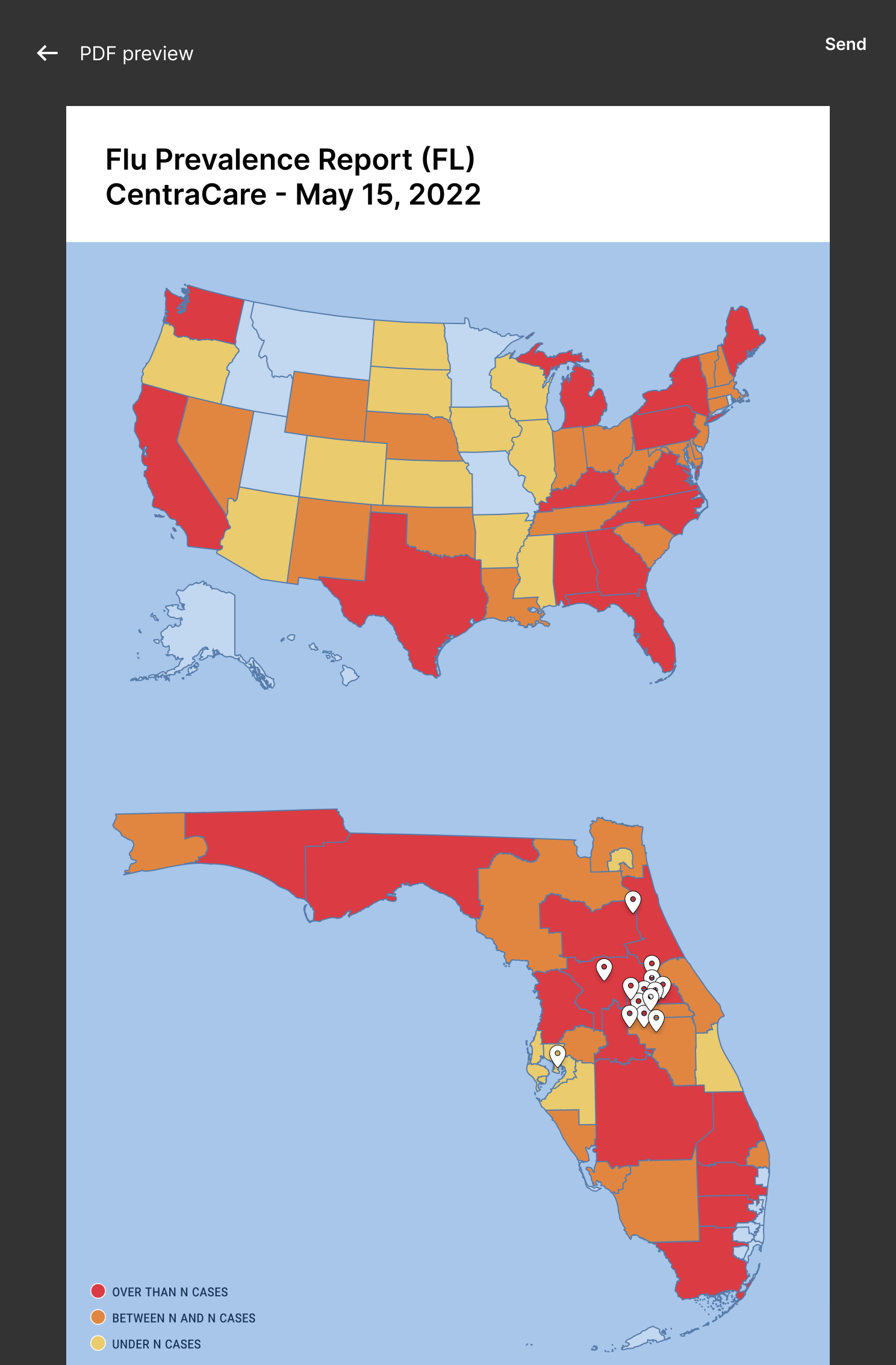
The same data, viewed differently. Status-over-time charts at the top — Total, Healthy, Critical, Needs Attention, Inactive — give engineers a system-level pulse before they drill down. Time-window filters (Week / 24h / 12h / 1h) let them shift between long-range planning and right-now triage. Device records are blurred to protect client privacy — the layout and design system are the work; the data belongs to Hologic.
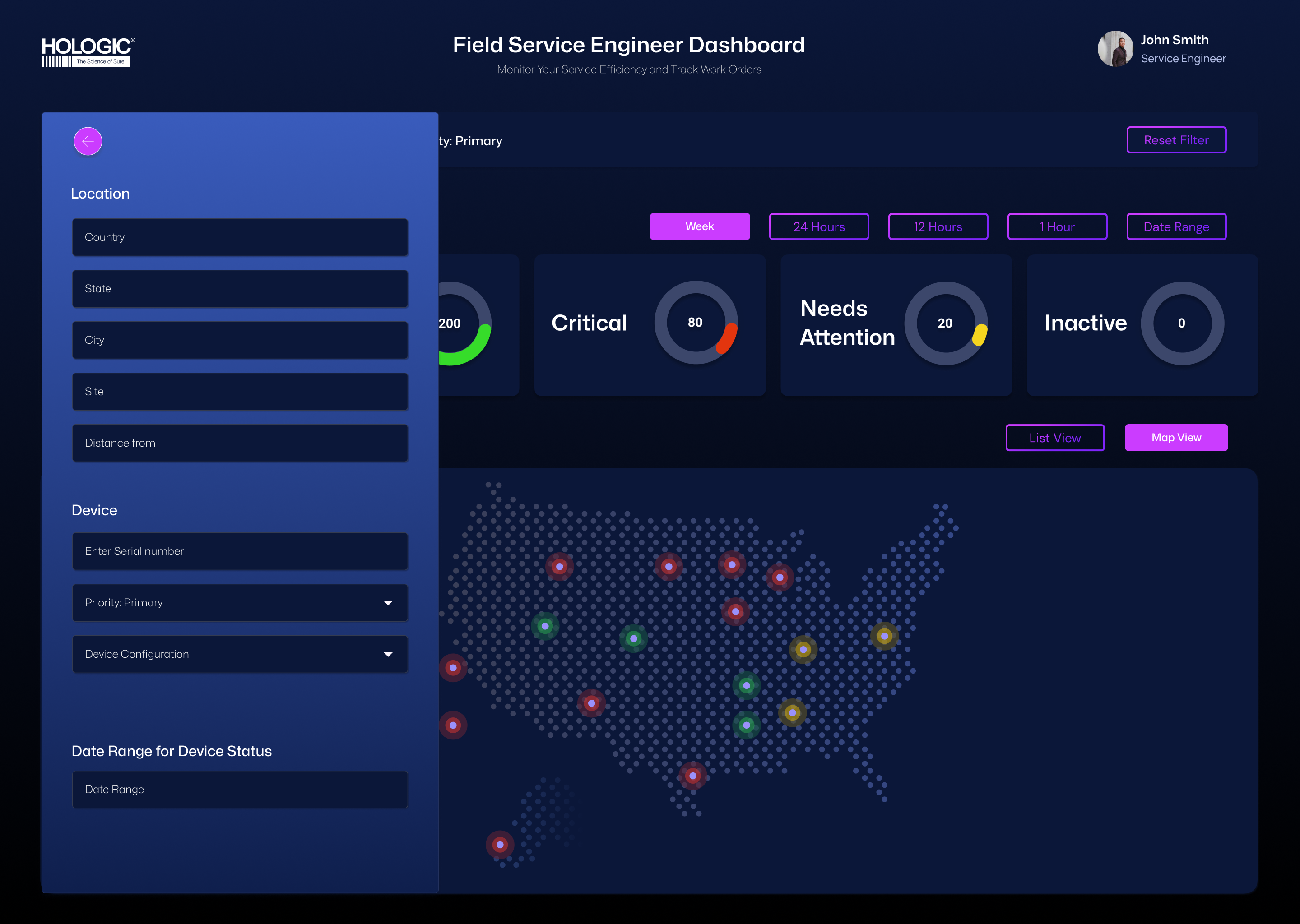
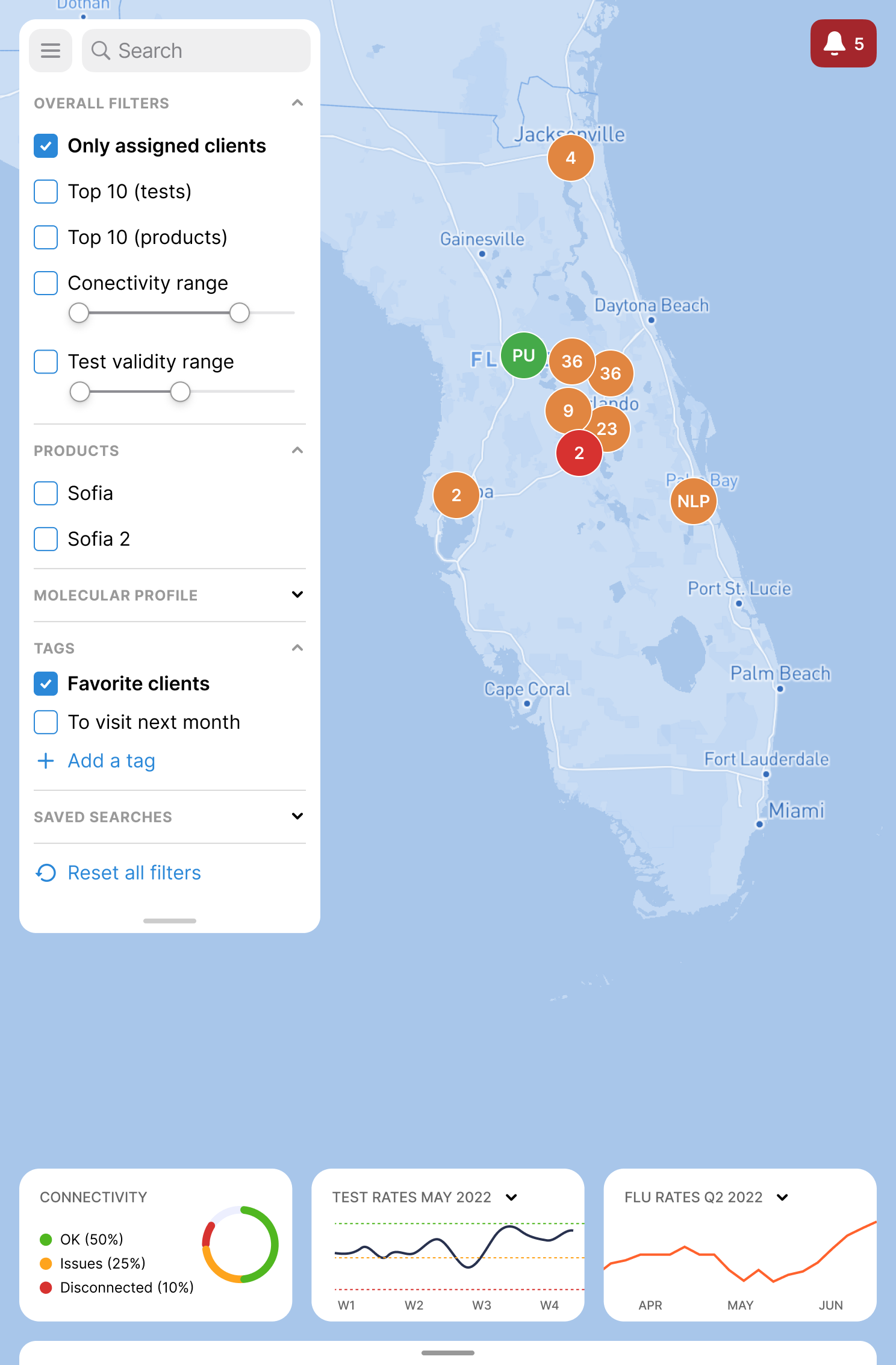
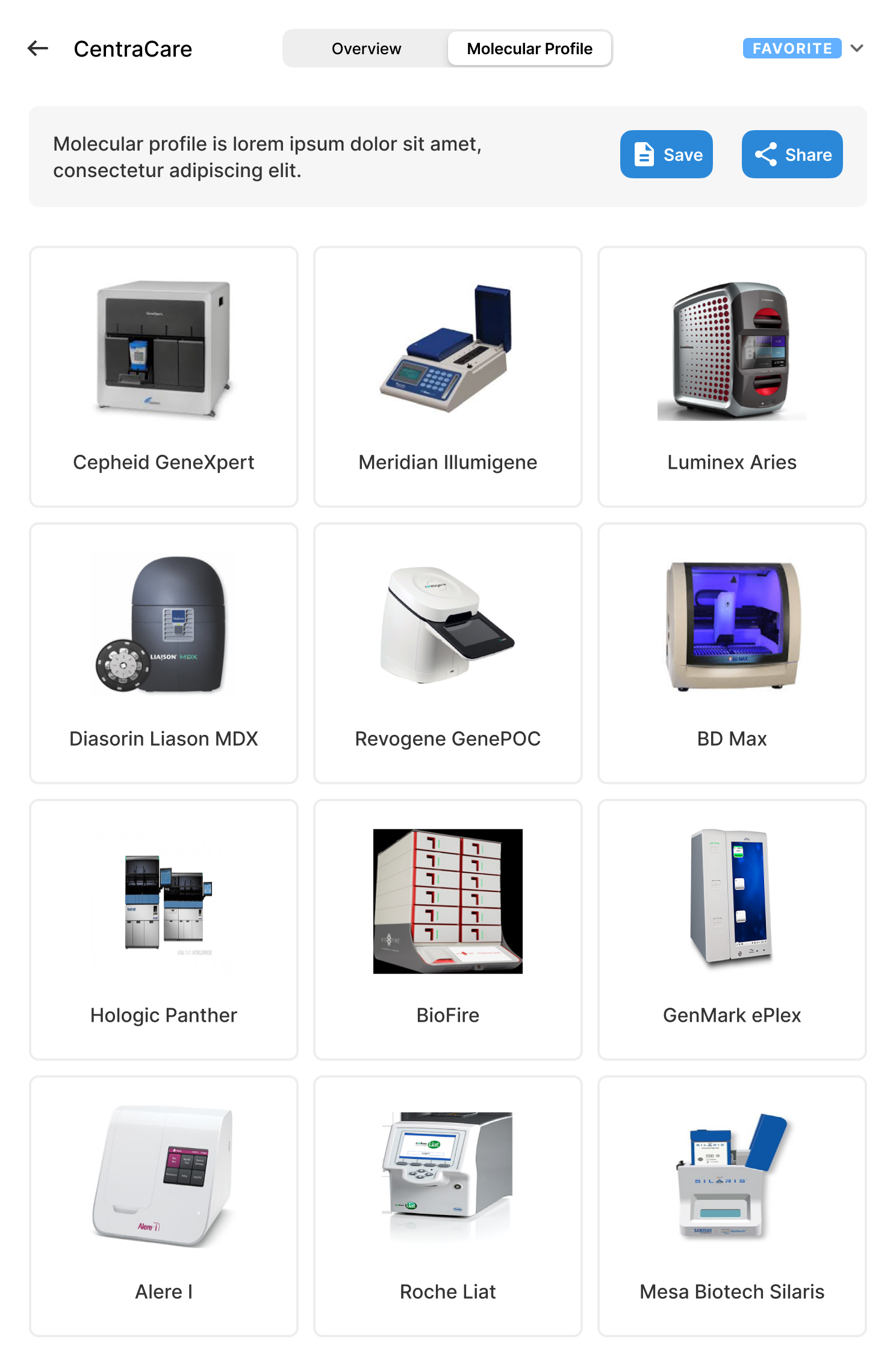
With hundreds of devices in play, filtering isn't a feature — it's the product. The slide-out filter panel groups controls into Location, Device, and Date Range, with sensible defaults (Priority: Primary) so engineers can get to a clean view in two clicks. The whole panel was designed to be keyboard-navigable for field engineers working hands-busy.
Two views, one truth
Map and list views share the same status logic and color system, so engineers can switch perspectives without recalibrating.
Color earns its meaning
Red is reserved for critical only. Yellow for warning. Green for healthy. No decoration. In healthcare, color is a signaling system, not a styling choice.
Status charts up top
Donut charts at the top of every view answer "what's the situation?" before a single record is loaded — saving FSEs scanning time on every visit.